
2018년 3월 29일 정오표 (3rd print에 대한 수정) download
AJCC Cancer Staging from Supplement Download :
AJCC 8th ed. cancer staging
2016년 10월 Springer출판사를 통해 AJCC 8th edition cancer staging manual이 발간이 되었다. “a bridge from Population-based to a more ‘personalized’ approach to cancer staging” 이라는 비젼을 걸고 진행된 프로젝트로 AJCC(American Joint Committee on Cancer)의 공식홈페이지(cancerstaging.org)에서는 원래 2017년 1월 1일 부터 적용하기로 한 새로운 병기설정시스템의 시행을 2018년 1월 1일로 연기 한다는 이야기와 함께, 2017년 12월 31일까지는 7판의 기준을 적용하는 것으로 공지하고 있다. 공식적으로는에러를 계속 수정하고 있지만, 그 오류가 심각하지는 않아2016년 말에 출판한 책자에 대해 새로 인쇄를 하지 않을 것이지만, API를 통한 전자등록 방법을 적용하기에 앞서 미국내 여러기관들 (National Cancer Institute (NCI-SEER), Centers for Disease Control and Prevention (CDC), the College of American Pathologists (CAP), the National Comprehensive Cancer Network (NCCN, the National Cancer Data Base (NCDB), and the Commission on Cancer (CoC))과 상의하여 실무적인 조율이 필요하다는 판단하에 2018년 1월부터 새로운 병기를 적용하는 것으로 결정하였다고 공지하고 있다. 여기서는 8판에서 바뀐 기준과 cancer staging의 paradigm shift에 대해 이야기하고자 한다.
(1) AJCC staging system
TNM 분류의 개념은 1940년대 Pierre Denoix에 의해 처음으로 개발되었다. 1959년에 결성된 AJCC는 1977년 처음으로 cancer staging manual을 출간하였다. 서론에서 스위스 제네바에 본부를 두고 있는 the International Union Against Cancer (Union Internationale Centre le Cancer, UICC) 에서 출판한 TNM classification of malignant tumor에 부합하여 분류체계를 만들려고 하였다고 기술하였으며 1983년 2판에서 UICC의 TNM committee에 의해 제란된 병기에 따라 구상하게 되었다. 2002년의 6판에서 몇가지의 비해부학적인 요소들을 추가하였고, 2009년 7판에서 더 많은 비해부학적인 표지자들을 확대하여 포함시키게 된다.
TNM system 에 의한 병기분류의 의의는
- readily communicated to others
- to assist in decisions regarding treatment
- to be a facor in judgement as to prognosis
- comparing like or unlike groups of cases
에 있기 때문에 초판에서 8판까지의 개정은 이전 분류법으로부터의 일관성을 유지하면서 데이터로부터 새로 발견된 요소들을 적용시키는 것의 균형을 잘 유지하는 것이 중요하다고 할 수 있다. 구강암은 다른 암에 비해 수술에 의한 치료의 비중이 높기 때문에 비교적 병리학적인 확인이 가능한 데이터가 많기 때문에 다른 암에 비해 표준적인 데이터를 많이 얻을 수 있는 장점을 지니고 있다.
8판에서는 18개의 Expert panel을 통해 해부학적인 부위별로 구분하여 진행한 결과를 기술하고 있다.
초판부터 두경부는 Oral cavity, Pharynx, Parynx, paranasal sinuses로 나뉘며, salivary gland, thyroid를 따로 분류하고 있다. 8판에서는 pharynx를 nasopharyngeal carcinoma(chapter 9), HR-HPV-associated(p16-positive) OPC(chapter 10), 그리고 hypopharyngeal and non-HR-HPV associated(p16-negative) OPC(chapter 11) 의 세 부분으로 다시 구분하고 있다.
| Edition | Publication Year | Effective Year |
| 1 | 1977 | 1978 |
| 2 | 1983 | 1984 |
| 3 | 1988 | 1989 |
| 4 | 1992 | 1993 |
| 5 | 1997 | 1998 |
| 6 | 2002 | 2003 |
| 7 | 2009 | 2010 |
| 8 | 2016 | 2018 |
(2) AJCC 8th edition – Head and Neck
8판의 대표적인 변화는 구인두암(Oropharyngeal cancer)에서 HR-HPV associated(p16+) cancer를 구분하여 병기를 나누고 있다는 것이다. 구강의 암(oral cavity cancer)의 경우에는 Depth of Invasion 을 병기에 포함을 시켰으며, 경부림프절 전이에서 extranodal extension(ENE)를 병기 구분에 포함시켰다. 또한 neoadjuvant therapy를 받은 환자의 경우 staging을 yc 혹은 yp를 이용한 별도의 staging을 하는 것을 추가하였다. 또한 API(Application Programming Interface)라는 시스템을 통해 staging manual 내용을 배포할 예정으로 있다.
1) Oral cavity cancer(OCC)
구강암에서의 T stage 개정은 DOI을 포함시켰다는 것과 T0가 삭제되었다는 것이다. 그동안 많은 연구에서 암종의 두꼐가 예후와 관련이 많다는 것이 알려졌다. 최근의 연구에서 DOI가 종양의 thickness보다 더 예측도가 높은 인자라는 것이 제안되었으며, 6판의 staging manual부터 DOI가 기록이 되어 분석이 가능하게 되었다. 의사의 임상적인 검사로도 less invasive(5mm 이하). Moderate depth(5 mm 초과 10 mm 이하), deeply invasive (10 mm초과)를 구분하는 것이 문제가 되지는 않는다. 병기 구분이 이제는 더이상 표면적인 크기만으로 구분되지는 않게 되었다. 병리적으로는 가장 가까운 정상 점막의 기저막 사이를 이은 선에서 가장 깊은 곳으로 수선을 그은 것으로 DOI을 표시한다. 병소에 따라 tumor thick ness가 DOI보다 클 수도 작을 수도 있다. 또한 T4에서 Extrinsic muscle의 침투가 기준으로 사용되지는 않는데 DOI에 의한 구분이 이것보다는 상위 혹은 더 중요하며, 근육의 침투를 임상적으로든 병리적으로든 평가하기가 쉽지 않기 때문이다.
T Category for Oral Cavity Cancer, 8th Edition Staging Manual
| T category | T criteria |
| TX | Primary tumor cannot be assessed |
| Tis | Carcinoma in situ |
| T1
|
Tumor ≤2 cm, ≤5 mm depth of invasion (DOI) (DOI is depth of invasion and not tumor thickness) |
| T2 | Tumor ≥2 cm, DOI >5 mm and ≤10 mm or tumor >2cm but ≤4 cm, and ≤10 mm DOI |
| T3 | Tumor >4cmor any tumor >10 mm DOI |
| T4 | Moderately advanced or very advanced local disease |
| T4a | Moderately advanced local disease: (lip) tumor invades through cortical bone or involves the inferior alveolar nerve, floor of mouth, or skin of face (ie, chin or nose); (oral cavity) tumor invades adjacent structures only (eg, through cortical bone of the mandible or maxilla, or involves the maxillary sinus or skin of the face); note that superficial erosion of bone/tooth socket (alone) by a gingival primary is not sufficient to classify a tumor as T4 |
| T4b | Very advanced local disease; tumor invades masticator space, pterygoid plates, or skull base and/or encases the internal carotid artery |
Regional Lymph Nodes Pathologic Category Criteria (pN)
| N CATEGORY | N CRITERIA |
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1
|
Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension and ENE-negative |
| N2 | |
| N2a
|
Metastasis in a single ipsilateral or contralateral lymph node 3 cm or less in greatest dimension and ENE-positive; or metastasis in a single ipsilateral lymph node more than 3 cm but not more than 6 cm in greatest dimension and ENE-negative |
| N2b | Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension and ENE-negative |
| N2c | Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension and ENE-negative |
| N3 | |
| N3a | Metastasis in a lymph node more than 6 cm in greatest dimension and ENE-negative |
| N3b
|
Metastasis in a single ipsilateral node more than 3 cm in greatest dimension and ENE-positive; or metastasis in multiple ipsilateral, contralateral, or bilateral lymph nodes, with any ENE-positive |
Note that a designation of “U” or “L” may be used for any N stage to indicate metastasis above the lower border of the cricoid (U) or below the lower border of the cricoid (L). Similarly, clinical and pathologic ENE should be recorded as ENE-negative or ENE-positive.
림프절 전이의 상태는 예후를 결정하는 중요한 인자이다. 전이림프절의 수와 크기와 함계 Extranodal extension 은 또하나의 예후의 변수이다. ENE가 예후에 영향을 미친다는 연구결과는 오랬동안 있어왔고 p16 +, HR-HPV-associated OPC는 예외라는 것이 알려졌다. 현재의 영상자료로는 초기의 최소한의 ENE를 확인하는 데 한계를 가지고 있는 것이 사실이다. 영상에서의 증거들은 ENE가 있다는 뒷바침은 될 수 있으나 충분하지는 않다. 병리적으로 밝혀진 ENE는 전이된 암조직이 림프절의 fibrous capsule을 뚫고 주변 결합조직으로 확장된 것으로 정의된다. Minor ENE(ENEmi)는 capsule에서 2mm이내인 경우로 정의되고 major ENE(ENEma) 육안으로도 뚫고 나와 있거나 2 mm 이상의 경우로 정의된다. 이러한 구분은 현재로서는 향후 자료로서의 데이터 수집으로만 사용되며, 현재는 둘 다 ENE+로 정의된다.
2) Oropharyngeal cancer(OPC)
HPV-associated(p16+) OPC 의 경우 Tis와 T4b 항목을 삭제하였다.
| Human Papillomavirus-Associated (p16-Positive) | Non-Human Papillomavirus-Associated (p16-Negative) | ||
| T category | T criteria | T category | T criteria |
| T0 | No primary identified | ||
| Tx | Primary tumor cannot be assessed | ||
| Tis | Carcinoma in situ | ||
| T1
|
Tumor 2 cm or smaller in greatest dimension | T1 | Tumor 2 cm or smaller in greatest dimension |
| T2 | Tumor larger than 2 cm but not larger than 4 cm in greatest dimension | T2 | Tumor larger than 2 cm but not larger than 4 cm in greatest dimension |
| T3 | Tumor larger than 4 cm in greatest dimension or extension to lingual surface of epiglottis | T3 | Tumor larger than 4 cm in greatest dimension or extension to lingual surface of epiglottis |
| T4 | Moderately advanced local disease; tumor invades the larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible or beyond | T4 | Moderately advanced or very advanced local disease
|
| T4a | Moderately advanced local disease; tumor invades the larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible | ||
| T4b | Very advanced local disease; tumor invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull base or encases carotid artery | ||
Anatomic Stage and Prognostic Groups for Clinical TNM Grouping of Human Papilloma virus-Associated (p16-Positive) Oropharyngeal Cancer, 8th Edition Staging Manuala

Anatomic Stage and Prognostic Groups for Clinical and Pathologic TNM Grouping of Non-Human Papillomavirus-Associated (p16-Negative) Oropharyngeal Cancer, 8th Edition Staging Manual

Clinical N Category Human Papillomavirus-Associated (p16-Positive) Oropharyngeal Cancer, 8th Edition Staging Manual
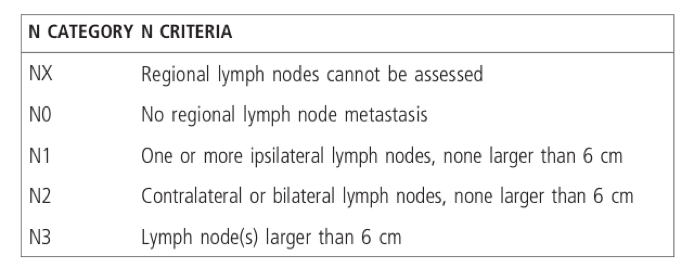
3) Unknown primary
원발병소가 발견되지 않은 림프절의 편평세포암이 Biopsy에서 밝혀지는 경우가 많다. 이런 환자들은 T0로 분류되었으나 원발부의 해부학적 부위가 특정되지 않안다. 최근에는 이러한 T0환자의 90%가 HR-HPV-associated cancer 로 나타났다. 임상적으로 원발부가 밝혀지지 않은 모든 경부림프절의 SCC는 HPV-ISH(In situ hybridization), p16 immunohistochemistry, EBER(Empstein-Barr-encoded RNA)-ISH 검사가 추전된다. 따라서, 이전의 AJCC분류와는 달리 Nasopharynx, HR-HPV-associated OPC, 그리고, salivary gland cancer를 제외한 다른 부위에서의 T0 를 삭제하였다.
(3) 병기구분법의 구강암 데이터에서의 확인
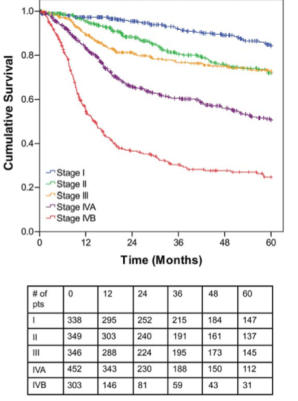
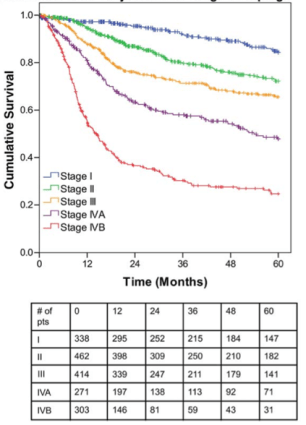
Memorial Sloan Kettering Cancer Center-Princess Margaret Hospital Institutional data를 이용하여 7판 TNM 분류와 8판 분류를 사용한 환자의 overall survival rate의 비교, 8판의 병기 구분(우측) 으로 stage II와 stage III이 더 확실히 구분가는 것을 볼 수 있다.
References
- Amin MB, Edge SB, Greene FL, et al, eds. AJCC Cancer Staging Manual. 8th ed. New York: Springer; 2017
- Lydiatt WM, Patel SG, O’Sullivan B, Brandwein MS, Ridge JA, Migliacci JC, et al. Head and Neck cancers-major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J Clin 2017; 67(2) : 122–137.
- Malm I-J, Fan CJ, Yin LX, Li DX, Koch WM, Gourin CG, et al. Evaluation of proposed staging systems for human papillomavirus-related oropharyngeal squamous cell carcinoma. Cancer 2017; 123(10) : 1768–1777.
- Lee C-C, Lin Y-S, Kang B-H, Chang K-P, Chi C-C, Lin M-Y, et al. Incorporation of log odds of positive lymph nodes into the AJCC TNM classification improves prediction of survival in oral cancer. Clin Otolaryngol 2017; 42(2) : 425–432.
- Mizumachi T, Homma A, Sakashita T, Kano S, Hatakeyama H, Fukuda S. Confirmation of the eighth edition of the AJCC/UICC TNM staging system for HPV-mediated oropharyngeal cancer in Japan. Int. J. Clin. Oncol. 2017; 18(Suppl 1) : 541–8.
